Overview
Coronary calcium scan
Coronary calcium scan
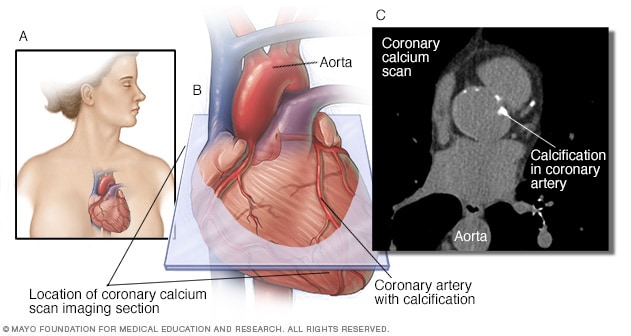
A coronary calcium scan uses computerized tomography (CT) imaging to take pictures of your heart's arteries. It can detect calcium deposits in the coronary arteries. Calcium deposits can narrow the arteries and increase the risk of a heart attack. The image on the left shows where the heart is typically located in the body (A). The middle image shows the area of the coronary calcium scan image (B). The image on the right shows a coronary calcium scan (C).
A coronary calcium scan is a special computerized tomography (CT) scan of the heart. It looks for calcium deposits in the heart arteries. A buildup of calcium can narrow the arteries and reduce blood flow to the heart. A coronary calcium scan may show coronary artery disease before you have symptoms.
Coronary calcium scan results can help determine the risk of heart attacks or strokes. Results from the scan may be used to plan or change treatment for coronary artery disease.
Other names for this test are:
- Coronary artery calcium (CAC) test.
- Coronary calcium CT scan.
- Heart CT calcium scan.
Products & Services
Why it's done
A coronary calcium scan is done to check for calcium in the arteries that supply the heart. It can help diagnose early coronary artery disease.
Coronary artery disease is a common heart condition. A buildup of calcium, fats and other substances in the heart arteries are often the cause. This buildup is called plaque. Plaque collects slowly over time, long before there are any symptoms of coronary artery disease.
A coronary calcium scan uses a series of X-rays to take pictures that can see if there's plaque that contains calcium.
This test might be done if:
- You have a strong family history of early coronary artery disease.
- Your risk for heart attacks is intermediate, not low or high.
- Your level of risk of heart attacks is uncertain.
A coronary calcium scan may help:
- Understand your risk of heart disease.
- Plan treatment if you have a low to moderate risk of heart disease or if your heart disease risk isn't clear.
A coronary calcium scan is not recommended as a general screening test for those known to be at high risk for heart attacks. It also isn't suggested if you have had a heart attack, a heart stent or coronary bypass surgery — because other tests or procedures that are done for those events show the heart arteries. Ask your health care team if a coronary calcium scan is right for you.
Risks
A coronary calcium scan uses X-rays. X-rays use radiation. The amount of radiation is generally considered safe.
Some medical centers advertise coronary calcium scans as an easy way to measure the risk of a heart attack. These scans often don't require a referral. But they might not be covered by insurance. Less expensive blood tests and blood pressure checks can help your health care team learn more about your heart attack risk. Ask your doctor what heart tests are best for you.
How you prepare
Do not smoke or use caffeine for a few hours before the test. Your health care team gives you specific instructions.
When you arrive for the test, you may be asked to change into a medical gown. Do not wear jewelry around your neck or near your chest.
What you can expect
During the procedure
Before a coronary calcium scan begins, sticky patches called electrodes are placed on your chest and sometimes your arms or legs. Wires connect the patches to a machine that checks your heartbeat.
The scan is done using a computerized tomography (CT) scanner. You lie on your back on a movable table. The table slides into a large machine shaped like a tube. Your head is outside the scanner the whole time. The exam room will likely be cool.
You may be given medicine to slow your heartbeat. This helps create clearer images. If you are nervous or anxious, you may get medicine to relax you.
You need to stay still while the pictures are taken. You may be asked to hold your breath for a few seconds. The health care professional doing the test can see and talk to you the entire time. The test takes about 10 to 15 minutes.
After the procedure
You usually can drive yourself home and continue your daily activities after the test unless your doctor tells you not to do so.
Results
Coronary calcium scan results are usually given as a number. The number is called the Agatston score. The score is the total area of calcium deposits and the density of the calcium.
- A score of zero means no calcium is seen in the heart. It suggests a low chance of developing a heart attack in the future.
- When calcium is present, the higher the score, the higher the risk of heart disease.
- A score of 100 to 300 means moderate plaque deposits. It's associated with a relatively high risk of a heart attack or other heart disease over the next 3 to 5 years.
- A score greater than 300 is a sign of more extensive disease and a higher heart attack risk.
The test score also may be given as a percentage. The number is the amount of calcium in the arteries compared to other people of the same age and sex. Calcium scores of about 75% have been linked with a significantly higher risk for heart attacks.
Discussing results with your health care team
Your health care team gives you your coronary calcium scan results. The result of a coronary calcium scan shouldn't be used as a single sign of your overall health and risk of heart disease. The information from the scan should be reviewed with other health information.
After a coronary calcium scan you may need one or more of the following plans:
- No change to your current treatment.
- A different medicine or dose of medicine.
- Changes to your diet and exercise routine.
- New weight-loss goals.
- More tests.
- Follow-up appointments to check your health and how well treatment is working.
If a coronary calcium scan shows calcium in the heart arteries, the test is not usually done again.
Clinical trials
Explore Mayo Clinic studies of tests and procedures to help prevent, detect, treat or manage conditions.