Overview
Hemorrhoids
Hemorrhoids
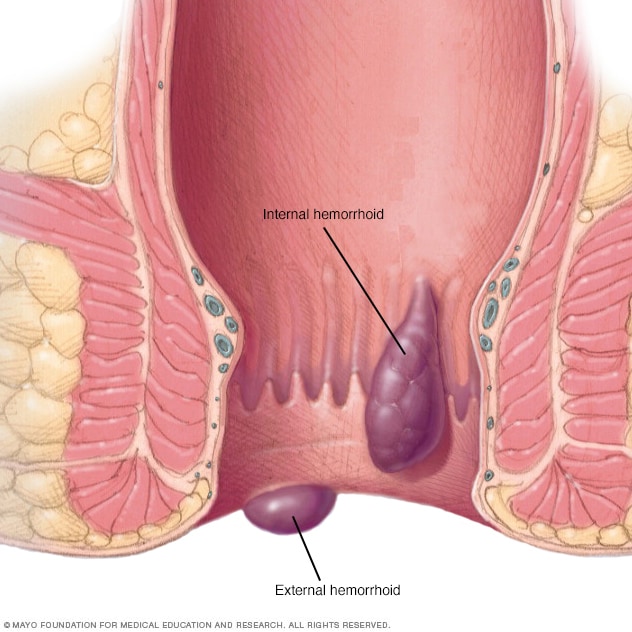
Hemorrhoids are swollen veins in your lower rectum. Hemorrhoids inside the rectum are usually painless but tend to bleed. Hemorrhoids outside the rectum may cause pain.
Hemorrhoids (HEM-uh-roids), also called piles, are swollen veins in the anus and lower rectum. Hemorrhoids are similar to varicose veins. Hemorrhoids can develop inside the rectum, called internal hemorrhoids. They also can develop under the skin around the anus, called external hemorrhoids.
There are several options available to treat hemorrhoids. Many people get relief with home treatments and lifestyle changes.
Symptoms
Symptoms of hemorrhoids usually depend on the type of hemorrhoid.
Internal hemorrhoids
Internal hemorrhoids lie inside the rectum. You usually can't see or feel them, and they rarely cause discomfort. But straining or irritation when passing stool can cause:
- Painless bleeding during bowel movements. You might notice small amounts of bright red blood on your toilet tissue or in the toilet.
- A hemorrhoid to push through the anal opening, called a prolapsed or protruding hemorrhoid. This may result in pain and irritation.
External hemorrhoids
These are under the skin around the anus. Symptoms might include:
- Itching or irritation in the anal region.
- Pain or discomfort.
- Swelling around the anus.
- Bleeding.
Thrombosed hemorrhoids
Blood can pool in an external hemorrhoid and form a clot, called a thrombus. A thrombosed hemorrhoid can result in:
- Severe pain.
- Swelling.
- Inflammation.
- A hard, discolored lump near the anus.
When to see a doctor
If you have bleeding during bowel movements or you have hemorrhoids that don't improve after a week of home care, talk to your health care provider.
Don't assume rectal bleeding is due to hemorrhoids, especially if you have changes in bowel habits or if your stools change in color or consistency. Rectal bleeding can happen with other diseases, including colorectal cancer and anal cancer.
Seek emergency care if you have large amounts of rectal bleeding, lightheadedness, dizziness or faintness.
Causes
The veins around the anus tend to stretch under pressure and may bulge or swell. Hemorrhoids can develop from increased pressure in the lower rectum due to:
- Straining during bowel movements.
- Sitting for long periods of time, especially on the toilet.
- Having chronic diarrhea or constipation.
- Being obese.
- Being pregnant.
- Having anal intercourse.
- Eating a low-fiber diet.
- Regularly lifting heavy items.
Risk factors
As people age, the risk of hemorrhoids increases. That's because the tissues that support the veins in the rectum and anus can weaken and stretch. This also can happen during pregnancy because the baby's weight puts pressure on the anal region.
Complications
Complications of hemorrhoids are rare but may include:
- Anemia. Rarely, ongoing blood loss from hemorrhoids may cause anemia. Anemia is when there aren't enough healthy red blood cells to carry oxygen to the body's cells.
- Strangulated hemorrhoid. When the blood supply to an internal hemorrhoid is cut off, the hemorrhoid is called strangulated. Strangulated hemorrhoids can cause extreme pain.
- Blood clot. Sometimes a clot can form in a hemorrhoid. This is called a thrombosed hemorrhoid. Although not dangerous, it can be extremely painful and sometimes needs to be drained.
Prevention
The best way to prevent hemorrhoids is to keep your stools soft so they pass easily. To prevent hemorrhoids and reduce symptoms of hemorrhoids, follow these tips:
- Eat high-fiber foods. Eat more fruits, vegetables and whole grains. Doing so softens the stool and increases its bulk. This will help you avoid the straining that can cause hemorrhoids. Add fiber to your diet slowly to avoid problems with gas.
- Drink plenty of fluids. Drink 6 to 8 glasses of water and other liquids each day to help keep stools soft. Avoiding alcohol also may help.
-
Consider fiber supplements. Most people don't get enough fiber in their diets. Studies have shown that nonprescription fiber supplements, such as psyllium (Metamucil, Konsyl, others) or methylcellulose (Citrucel), can lessen symptoms and bleeding from hemorrhoids.
If you use fiber supplements, be sure to drink at least eight glasses of water or other fluids every day. Otherwise, the supplements can cause constipation or make it worse.
- Don't strain. Straining and holding your breath when trying to pass stool create greater pressure in the veins in the lower rectum.
- Exercise. Stay active to help prevent constipation and reduce pressure on veins. Exercise also can help you lose excess weight that might be causing your hemorrhoids or making them worse.
- Avoid long periods of sitting. Sitting too long, especially on the toilet, can increase the pressure on the veins in the anus.
Aug. 25, 2023