Overview
Invasive lobular carcinoma is a type of breast cancer that begins in the milk-producing glands (lobules) of the breast.
Invasive cancer means the cancer cells have broken out of the lobule where they began and have the potential to spread to the lymph nodes and other areas of the body.
Invasive lobular carcinoma makes up a small portion of all breast cancers. The most common type of breast cancer begins in the breast ducts (invasive ductal carcinoma).
Products & Services
Symptoms
At its earliest stages, invasive lobular carcinoma may cause no signs and symptoms. As it grows larger, invasive lobular carcinoma may cause:
- An area of thickening in part of the breast
- A new area of fullness or swelling in the breast
- A change in the texture or appearance of the skin over the breast, such as dimpling or thickening
- A newly inverted nipple
Invasive lobular carcinoma is less likely than other forms of breast cancer to cause a firm or distinct breast lump.
When to see a doctor
Make an appointment with your doctor if you have any signs or symptoms that worry you. Your doctor will perform an examination and determine whether you need a diagnostic breast X-ray (mammogram) or a breast ultrasound.
Ask your doctor when to begin screening tests for breast cancer to help detect cancer early and before you may have any signs or symptoms. Routine screening tests may include a physical exam and a mammogram.
Various organizations differ on their screening recommendations, but many suggest women with an average risk of breast cancer consider beginning mammograms in their 40s.
If you have a family history of breast cancer or other factors that increase your risk of breast cancer, your doctor may recommend beginning screening mammograms or other tests at an earlier age.
Causes
Breast anatomy
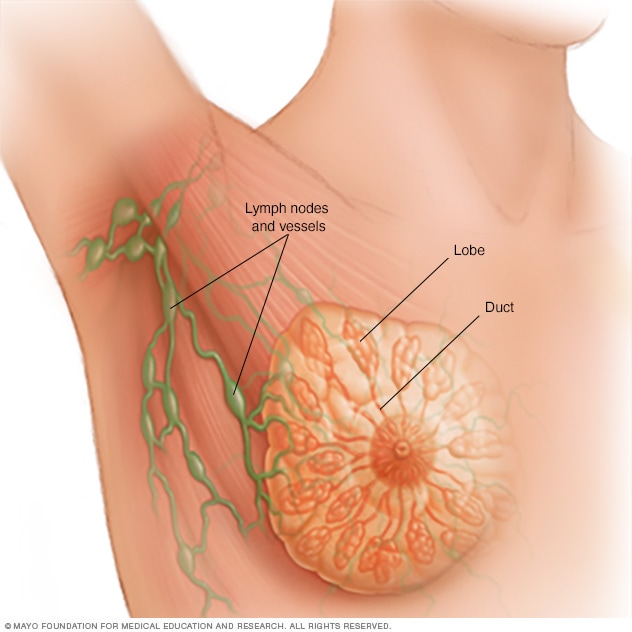
Breast anatomy
Each breast contains 15 to 20 lobes of glandular tissue, arranged like the petals of a daisy. The lobes are further divided into smaller lobules that produce milk for breastfeeding. Small tubes, called ducts, conduct the milk to a reservoir that lies just beneath your nipple.
It's not clear what causes invasive lobular carcinoma.
Doctors know that invasive lobular carcinoma begins when cells in one or more milk-producing glands of the breast develop mutations in their DNA. The mutations lead to the inability to control cell growth, which results in the cells dividing and growing rapidly. Depending on the aggressiveness of the cancer type, the cancer cells can spread to other parts of the body.
Lobular carcinoma cells tend to invade breast tissue by spreading out in a distinct way rather than forming a firm nodule. The affected area may have a different feel from the surrounding breast tissue, more like a thickening and fullness, but it's unlikely to feel like a lump.
Risk factors
Factors that may increase your risk of invasive lobular carcinoma include:
- Being female. Women are more likely to develop breast cancer, but men also can develop breast cancer.
- Older age. Your risk of breast cancer increases as you age. Women with invasive lobular carcinoma tend to be a few years older than women diagnosed with other types of breast cancer.
- Lobular carcinoma in situ (LCIS). If you've been diagnosed with LCIS — abnormal cells confined within breast lobules — your risk of developing invasive cancer in either breast is increased. LCIS isn't cancer, but is an indication of increased risk of breast cancer of any type.
- Postmenopausal hormone use. Use of the female hormones estrogen and progesterone during and after menopause has been shown to increase the risk of invasive lobular carcinoma.
-
Inherited genetic cancer syndromes. Women with a rare inherited condition called hereditary diffuse gastric cancer syndrome have an increased risk of both stomach (gastric) cancer and invasive lobular carcinoma.
Women with certain inherited genes may have an increased risk of breast and ovarian cancers.
Prevention
To reduce your risk of breast cancer, consider trying to:
-
Discuss the benefits and risks of menopausal hormone therapy with your doctor. Combination hormone therapy may increase the risk of breast cancer.
Some women experience bothersome signs and symptoms during menopause and, for these women, the increased risk of breast cancer may be acceptable in order to relieve menopause signs and symptoms.
To reduce the risk of breast cancer, use the lowest dose of hormone therapy possible for the shortest amount of time.
- Drink alcohol in moderation, if at all. If you choose to drink alcohol, do so in moderation. For healthy adults, that means up to one drink a day for women of all ages and men older than age 65, and up to two drinks a day for men age 65 and younger.
- Exercise most days of the week. Aim for at least 30 minutes of exercise on most days of the week. If you haven't been active lately, ask your doctor whether exercise is OK and then start slowly.
-
Maintain a healthy weight. If your current weight is healthy, work to maintain that weight.
If you need to lose weight, ask your doctor about healthy weight-loss strategies. Reduce the number of calories you eat each day and slowly increase the amount of exercise. Aim to lose weight slowly — about 1 or 2 pounds a week.
If you have a family history of breast cancer or feel you may have an increased risk of breast cancer, discuss it with your health care provider. Preventive medications, surgery and more-frequent screening may be options for women with a high risk of breast cancer.