Overview
Parts of the throat (pharynx)
Parts of the throat (pharynx)
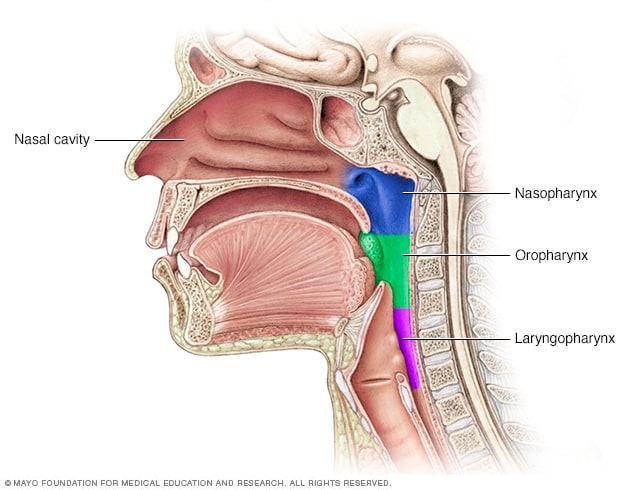
The throat (pharynx) is a muscular tube that runs from the back of your nose down into your neck. It contains three sections: the nasopharynx, oropharynx and laryngopharynx, which is also called the hypopharynx.
Nasopharyngeal (nay-zoh-fuh-RIN-jee-ul) carcinoma is cancer that occurs in the nasopharynx, which is located behind your nose and above the back of your throat.
Nasopharyngeal carcinoma is rare in the United States. It occurs much more frequently in other parts of the world — specifically Southeast Asia.
Nasopharyngeal carcinoma is difficult to detect early. That's probably because the nasopharynx isn't easy to examine and symptoms of nasopharyngeal carcinoma mimic those of other, more-common conditions.
Treatment for nasopharyngeal carcinoma usually involves radiation therapy, chemotherapy or a combination of the two. You can work with your doctor to determine the exact approach depending on your particular situation.
Products & Services
Symptoms
In its early stages, nasopharyngeal carcinoma may not cause any symptoms. Possible noticeable symptoms of nasopharyngeal carcinoma include:
- A lump in your neck caused by a swollen lymph node
- Blood in your saliva
- Bloody discharge from your nose
- Nasal congestion or ringing in your ears
- Hearing loss
- Frequent ear infections
- Sore throat
- Headaches
When to see a doctor
Early nasopharyngeal carcinoma symptoms may not always prompt you to see your doctor. However, if you notice any unusual and persistent changes in your body that don't seem right to you, such as unusual nasal congestion, see your doctor.
Causes
Cancer begins when one or more genetic mutations cause normal cells to grow out of control, invade surrounding structures and eventually spread (metastasize) to other parts of the body. In nasopharyngeal carcinomas, this process begins in the squamous cells that line the surface of the nasopharynx.
Exactly what causes the gene mutations that lead to nasopharyngeal carcinoma isn't known, though factors, such as the Epstein-Barr virus, that increase the risk of this cancer have been identified. However, it isn't clear why some people with all the risk factors never develop cancer, while others who have no apparent risk factors do.
Risk factors
Researchers have identified some factors that appear to increase your risk of developing nasopharyngeal carcinoma, including:
- Sex. Nasopharyngeal carcinoma is more common in men than it is in women.
- Race. This type of cancer more commonly affects people in parts of China, Southeast Asia and northern Africa. In the United States, Asian immigrants have a higher risk of this type of cancer than do American-born Asians. Inuits in Alaska also have an increased risk of nasopharyngeal cancer.
- Age. Nasopharyngeal cancer can occur at any age, but it's most commonly diagnosed in adults between the ages of 30 and 50.
- Salt-cured foods. Chemicals released in steam when cooking salt-cured foods, such as fish and preserved vegetables, may enter the nasal cavity, increasing the risk of nasopharyngeal carcinoma. Being exposed to these chemicals at an early age may increase the risk even more.
- Epstein-Barr virus. This common virus usually produces mild signs and symptoms, such as those of a cold. Sometimes it can cause infectious mononucleosis. The Epstein-Barr virus is also linked to several rare cancers, including nasopharyngeal carcinoma.
- Family history. Having a family member with nasopharyngeal carcinoma increases your risk of the disease.
- Alcohol and tobacco. Heavy alcohol intake and tobacco use can raise your risk of developing nasopharyngeal carcinoma.
Complications
Nasopharyngeal carcinoma complications can include:
- Cancer that grows to invade nearby structures. Advanced nasopharyngeal carcinoma can cause complications if it grows large enough to invade nearby structures, such as the throat, bones and brain.
-
Cancer that spreads to other areas of the body. Nasopharyngeal carcinoma frequently spreads (metastasizes) beyond the nasopharynx.
Most people with nasopharyngeal carcinoma have regional metastases. That means cancer cells from the initial tumor have migrated to nearby areas, such as lymph nodes in the neck.
Cancer cells that spread to other areas of the body (distant metastases) most commonly travel to the bones, lungs and liver.
Prevention
No sure way exists to prevent nasopharyngeal carcinoma. However, if you're concerned about your risk of nasopharyngeal carcinoma, you may consider avoiding habits that have been associated with the disease. For instance, you may choose to cut back on the amount of salt-cured foods you eat or avoid these foods altogether.
Tests to screen for nasopharyngeal carcinoma
In the United States and in other areas where the disease is rare, routine screening for nasopharyngeal carcinoma isn't done.
But in areas of the world where nasopharyngeal carcinoma is much more common — for instance, in some areas of China — doctors may offer screenings to people thought to be at high risk of the disease. Screening may involve blood tests to detect the Epstein-Barr virus.
Sept. 08, 2022