Overview
Sciatic nerve

Sciatic nerve
The sciatic nerve is the confluence of nerve roots from the lower back. The sciatic nerve extends from the buttocks down each leg.
Sciatica refers to pain that travels along the path of the sciatic nerve. The sciatic nerve travels from the buttocks and down each leg.
Sciatica most often happens when a herniated disk or an overgrowth of bone puts pressure on the lumbar spine nerve roots. This happens "upstream" from the sciatic nerve. This causes inflammation, pain and often some numbness in the affected leg.
Although the pain associated with sciatica can be serious, those cases that are caused by a herniated disk can clear up with treatment in a few weeks to months. People who have severe sciatica and serious leg weakness or bowel or bladder changes might need surgery.
Symptoms
Sciatica pain can be almost anywhere along the nerve pathway. It's especially likely to follow a path from the low back to the buttock and the back of a thigh and calf.
The pain can vary from a mild ache to a sharp, burning pain. Sometimes it feels like a jolt or electric shock. It can be worse when coughing or sneezing or sitting a long time. Usually, sciatica affects only one side of the body.
Some people also have numbness, tingling, or muscle weakness in the leg or foot. One part of the leg can be in pain, while another part can feel numb.
When to see a doctor
Mild sciatica usually goes away over time. Call your primary care professional if self-care measures don't ease symptoms. Also call if pain lasts longer than a week, is severe or gets worse. Get immediate medical care for:
- Sudden numbness or muscle weakness in a leg.
- Pain after a violent injury, such as a traffic accident.
- Trouble controlling bowels or bladder.
Causes
Herniated disk
Herniated disk
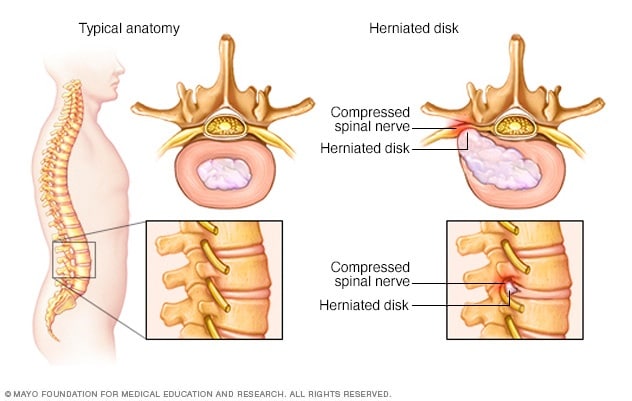
The disks that lie between the vertebrae in the spine consist of a soft center (nucleus) surrounded by a tougher exterior (annulus). A herniated disk occurs when a portion of the nucleus pushes through a crack in the annulus. Symptoms may occur if the herniation compresses a nerve.
Sciatica occurs when the nerve roots to the sciatic nerve become pinched. The cause is usually a herniated disk in the spine or an overgrowth of bone, sometimes called bone spurs, on the spinal bones. More rarely, a tumor can put pressure on the nerve.
Risk factors
Risk factors for sciatica include:
- Age. People ages 20 to 50 are most likely to have herniated disks. Bone spurs develop more commonly as people age.
- Obesity. Being overweight increases stress on the spine.
- Occupation. A job that requires twisting the back, carrying heavy loads or driving a motor vehicle for long periods might play a role in herniated disks.
- Prolonged sitting. People who sit a lot or don't move much are more likely to develop herniated disks than active people are.
- Diabetes. This condition, which affects the way the body uses blood sugar, increases the risk of nerve damage.
Complications
Most people recover fully from sciatica caused by herniated disks, often without treatment. But sciatica can damage nerves. Seek immediate medical attention for:
- Loss of feeling in the affected leg.
- Weakness in the affected leg.
- Loss of bowel or bladder control.
Prevention
It's not always possible to prevent sciatica, and the condition can come back. To protect your back:
- Exercise regularly. To keep the back strong, work the core muscles — the muscles in the abdomen and lower back needed for good posture and alignment. A healthcare professional can recommend activities.
- Keep good posture when sitting. Choose a seat with good lower back support, armrests and a swivel base. For better low back support, place a pillow or rolled towel in the small of the back to keep its normal curve. Keep knees and hips level.
- Use your body correctly. When standing for long periods, rest one foot on a stool or small box from time to time. When lifting something heavy, let your legs do the work. Hold the load close to your body. Don't lift and twist at the same time. Find someone to help lift heavy or awkward things.
Jan. 31, 2024