Overview
Thyroid nodules are solid or fluid-filled lumps that form within your thyroid, a small gland located at the base of your neck, just above your breastbone.
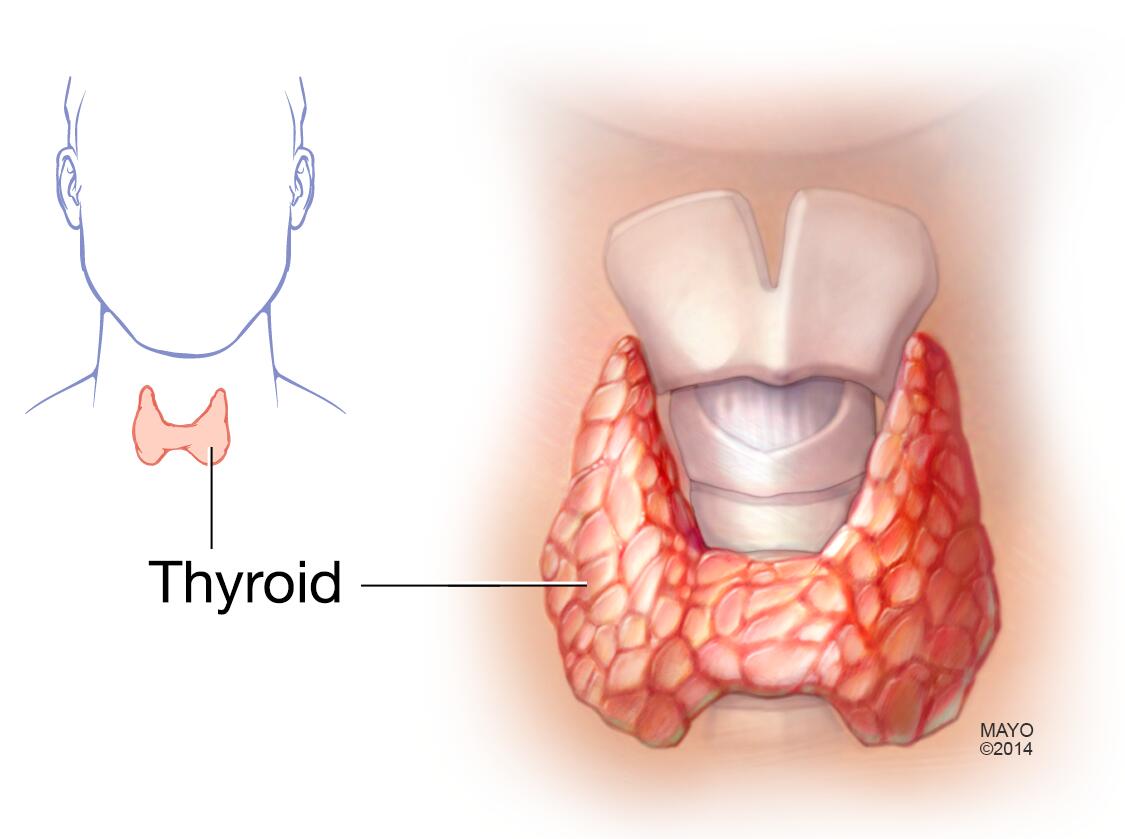
Thyroid gland
The thyroid gland is located at the base of the neck, just below the Adam's apple.
Most thyroid nodules aren't serious and don't cause symptoms. Only a small percentage of thyroid nodules are cancerous.
You often won't know you have a thyroid nodule until your doctor discovers it during a routine medical exam. Or your doctor may uncover it during a scan that was done for another health reason. Some thyroid nodules, however, may become large enough to be visible or make it difficult to swallow or breathe.
Treatment options depend on the type of thyroid nodule you have.
Symptoms
Most thyroid nodules don't cause signs or symptoms. But occasionally some nodules become so large that they can:
- Be felt
- Be seen, often as a swelling at the base of your neck
- Press on your windpipe or esophagus, causing shortness of breath or difficulty swallowing
In some cases, thyroid nodules produce additional thyroxine, a hormone secreted by your thyroid gland. The extra thyroxine can cause symptoms of an overproduction of thyroid hormones (hyperthyroidism), such as:
- Unexplained weight loss
- Increased sweating
- Tremor
- Nervousness
- Rapid or irregular heartbeat
Only a small number of thyroid nodules are cancerous. But determining which nodules are cancerous can't be done by evaluating your symptoms alone. Most cancerous thyroid nodules are slow growing and may be small when your doctor discovers them. Aggressive thyroid cancers are rare with nodules that may be large, firm, fixed and rapid growing.
When to see a doctor
Although most thyroid nodules are noncancerous and don't cause problems, ask your doctor to evaluate any unusual swelling in your neck, especially if you have trouble breathing or swallowing. It's important to evaluate the possibility of cancer.
Seek medical care if you develop signs and symptoms of hyperthyroidism, such as:
- Sudden weight loss even though your appetite is normal or has increased
- A pounding heart
- Trouble sleeping
- Muscle weakness
- Nervousness or irritability
Also see your doctor if you have signs and symptoms that may mean your thyroid gland isn't making enough thyroid hormone (hypothyroidism), which include:
- Feeling cold
- Feeling tired more easily
- Dry skin
- Memory problems
- Depression
- Constipation
From Mayo Clinic to your inbox
Causes
Several conditions can cause nodules to develop in your thyroid gland, including:
-
Overgrowth of normal thyroid tissue. An overgrowth of normal thyroid tissue is sometimes referred to as a thyroid adenoma. It's unclear why this occurs, but it's not cancerous and isn't considered serious unless it causes bothersome symptoms from its size.
Some thyroid adenomas lead to hyperthyroidism.
- Thyroid cyst. Fluid-filled cavities (cysts) in the thyroid most commonly result from degenerating thyroid adenomas. Often, solid components are mixed with fluid in thyroid cysts. Cysts are usually noncancerous, but they occasionally contain cancerous solid components.
- Chronic inflammation of the thyroid. Hashimoto's disease, a thyroid disorder, can cause thyroid inflammation and result in enlarged nodules. This often is associated with hypothyroidism.
- Multinodular goiter. The term goiter is used to describe any enlargement of the thyroid gland, which can be caused by iodine deficiency or a thyroid disorder. A multinodular goiter contains multiple distinct nodules within the goiter, but its cause is less clear.
-
Thyroid cancer. The chances that a nodule is cancerous are small. However, a nodule that is large and hard or causes pain or discomfort is more worrisome. You will likely want to have it checked by your doctor.
Certain factors increase your risk of thyroid cancer, such as a family history of thyroid or other endocrine cancers and having a history of radiation exposure from medical therapy or from nuclear fallout.
- Iodine deficiency. Lack of iodine in your diet can sometimes cause your thyroid gland to develop thyroid nodules. But iodine deficiency is uncommon in the United States, where iodine is routinely added to table salt and other foods.

Thyroid nodules
Enlargement of the thyroid can expand the gland well beyond its typical size and cause a noticeable bulge in the neck. This can be caused by single or multiple nodules (lumps) in the thyroid or by an autoimmune process.
Complications
Complications associated with some thyroid nodules include:
- Problems swallowing or breathing. Large nodules or a multinodular goiter can interfere with swallowing or breathing.
-
Hyperthyroidism. Problems can occur when a nodule or goiter produces thyroid hormone, leading to an excess amount of the hormone in the body. Hyperthyroidism can result in weight loss, muscle weakness, heat intolerance, and anxiousness or irritability.
Potential complications of hyperthyroidism include an irregular heartbeat, weak bones and thyrotoxic crisis, a rare but potentially life-threatening intensification of signs and symptoms that requires immediate medical care.
- Problems related to thyroid nodule surgery. If your doctor recommends surgery to remove a nodule, you may need to take thyroid hormone replacement therapy for the rest of your life.



