Overview
Prostate gland
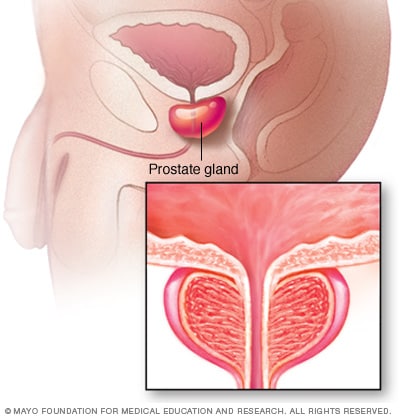
Prostate gland
The prostate gland is located just below the bladder in men and surrounds the top portion of the tube that drains urine from the bladder (urethra). The prostate's primary function is to produce the fluid that nourishes and transports sperm (seminal fluid).
Transurethral microwave thermotherapy (TUMT) is an outpatient procedure to treat urinary symptoms caused by an enlarged prostate, a condition known as benign prostatic hyperplasia (BPH). TUMT is generally considered a safe procedure with a low risk of side effects. It's generally used for men with other health conditions for whom more invasive surgery isn't recommended.
A small microwave antenna is inserted through the tip of the penis into the tube that carries urine from the bladder (urethra). Your doctor extends the antenna until it reaches the area of the urethra surrounded by the prostate. The antenna emits a dose of microwave energy that heats and destroys the excess prostate tissue that is blocking urine flow.
TUMT is one of several minimally invasive treatment options for BPH. To determine the right treatment for you, your doctor will consider the severity of your symptoms, any other health problems you have, and the size and shape of your prostate.
Products & Services
Why it's done
TUMT helps reduce urinary symptoms caused by BPH, including:
- Frequent, urgent need to urinate
- Difficulty starting urination
- Slow (prolonged) urination
- Increased frequency of urination at night
- Stopping and starting again while urinating
- The feeling you can't completely empty your bladder
- Urinary tract infections
TUMT can offer advantages over other methods of treating BPH, such as transurethral resection of the prostate (TURP) and open prostatectomy. The advantages might include:
- Lower risk of bleeding. TUMT can be a good option for men who take medication to thin their blood or who have a bleeding disorder that doesn't allow their blood to clot normally.
- No hospital stay. TUMT is generally done on an outpatient basis and might be a safer option than surgery if you have certain other health problems.
- Lower risk of dry orgasm. TUMT is less likely than some other BPH treatments to cause the release of semen into the bladder during ejaculation instead of out the body through the penis (retrograde ejaculation). Retrograde ejaculation isn't harmful but can interfere with your ability to father a child.
Risks
TUMT is generally safe with few if any major complications. Possible risks of TUMT might include:
- New onset or worsening urinary symptoms. Sometimes TUMT can result in chronic inflammation within the prostate. The inflammation can cause symptoms such as a frequent or urgent need to urinate, and painful urination.
- Temporary difficulty urinating. You might have trouble urinating for a few days after the procedure. Until you can urinate on your own, you will need to have a tube (catheter) inserted into your penis to carry urine out of your bladder.
- Urinary tract infection. This type of infection is a possible complication after any prostate procedure. An infection is increasingly likely to occur the longer you have a catheter in place. You will likely need antibiotics to treat the infection.
- Need for re-treatment. TUMT might be less effective in the treatment of urinary symptoms than other minimally invasive treatments or surgery. You might need to be treated again with another BPH therapy.
Because of potential complications, TUMT might not be a treatment option if you have or have had:
- A penile implant
- Narrowing of the urethra (urethral stricture)
- Certain types of BPH treatment affecting a specific area of the prostate (median lobe)
- A pacemaker or defibrillator
- Metal implants in the pelvic area, such as a total hip replacement
If you have other conditions that increase your risk of bleeding or if you take blood thinners — such as warfarin (Jantoven) or clopidogrel (Plavix) — your doctor may recommend a different procedure to treat your urinary symptoms.
How you prepare
Food and medications
You may be prescribed an antibiotic to prevent a urinary tract infection.
Other precautions
Arrange transportation home. You won't be able to drive after the procedure that day or generally if you have a catheter in your bladder.
You might not be able to work or do strenuous activity for 3 to 5 days after surgery. Ask your doctor how much recovery time you might need.
What you can expect
Transurethral microwave thermotherapy (TUMT)

Transurethral microwave thermotherapy (TUMT)
Transurethral microwave thermotherapy (TUMT) uses heat to destroy excess prostate tissue.
You'll be given a local anesthetic to numb the prostate area. The anesthetic might be inserted through the tip of your penis, or given in a shot via your rectum or in the area between your scrotum and anus.
You might also have intravenous (IV) sedation. With IV sedation, you'll be drowsy but remain conscious during the procedure.
During the procedure
Your doctor inserts a catheter with a microwave antenna into your urethra through the tip of your penis. A thermometer inserted into your rectum checks temperature. The antenna and thermometer have balloons attached that hold them in place. Your doctor might check the placement of the catheter and the rectal thermometer using an ultrasound machine.
During the procedure, the microwave antenna causes just enough heat to destroy the prostate tissue blocking your urine flow, but not enough to damage other tissue. Water circulating around the tip and sides of the antenna protects the urethra from heat. But you might feel some heat and discomfort in the prostate and bladder areas.
Your doctor will ask about your pain level and adjust your treatment to make sure you're getting enough heat to improve your symptoms. You'll need to stay as still as possible during the microwave treatment. The length of treatment time varies depending on your doctor's preference and the type of microwave therapy machine used.
During treatment, you might have a strong desire to urinate and may feel bladder spasms — sensations that usually go away after the treatment is finished.
After the procedure
Most men can go home the same day after the procedure, and recover in just a few days. You'll likely have a urinary catheter in place because of swelling that blocks urine flow. You may need to take antibiotics to prevent a urinary tract infection.
You might notice:
- Blood in your urine. This shouldn't last for more than a few days.
- Irritating urinary symptoms. You might feel an urgent or frequent need to urinate, or you might have to get up more often during the night to urinate. Most men experience burning, especially at the tip of the penis and near the end of urination. These symptoms generally last about a week.
- Difficulty holding urine. Incontinence can occur because your bladder is used to having to push urine through a urethra narrowed by enlarged prostate tissue. For most men, this issue improves with time.
- Urinary tract infection. Urinary tract infections are a possible complication after any enlarged prostate procedure. The risk of infection increases the longer you have a catheter in place.
Results
It might take several weeks to months for you to experience noticeable improvement in urinary symptoms. Your body needs time to break down and absorb overgrown prostate tissue that's been destroyed by microwave energy.
After TUMT, it's important to have a digital rectal exam once a year to check your prostate and screen for prostate cancer, as you would normally. If you notice any worsening urinary symptoms, see your doctor. Some men need re-treatment.
Sept. 09, 2023