Overview
Thyroid gland

Thyroid gland
The thyroid gland is located at the base of the neck, just below the Adam's apple.
Graves' disease is an immune system disorder that results in the overproduction of thyroid hormones (hyperthyroidism). Although a number of disorders may result in hyperthyroidism, Graves' disease is a common cause.
Thyroid hormones affect many body systems, so signs and symptoms of Graves' disease can be wide ranging. Although Graves' disease may affect anyone, it's more common among women and in people younger than age 40.
The primary treatment goals are to reduce the amount of thyroid hormones that the body produces and lessen the severity of symptoms.
Products & Services
Symptoms
Enlarged thyroid
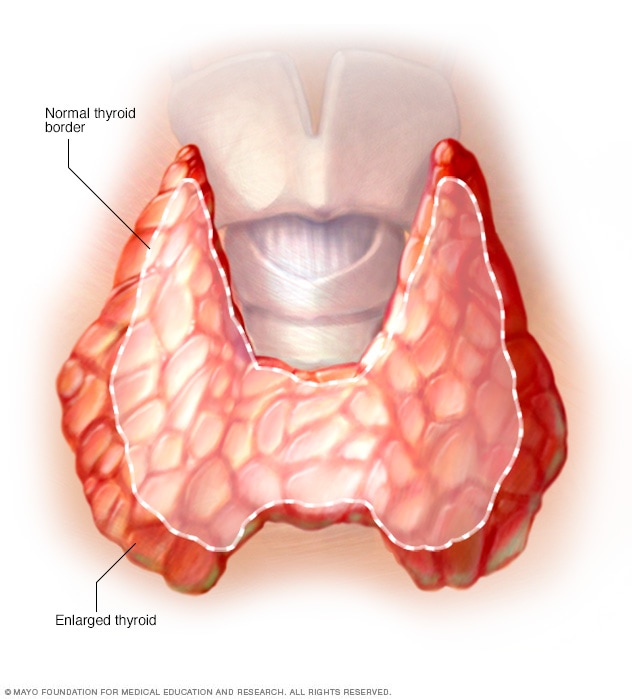
Enlarged thyroid
Widespread enlargement of the thyroid can expand the gland well beyond its typical size (left) and cause a noticeable bulge in the neck (right).
Common signs and symptoms of Graves' disease include:
- Anxiety and irritability
- A fine tremor of the hands or fingers
- Heat sensitivity and an increase in perspiration or warm, moist skin
- Weight loss, despite normal eating habits
- Enlargement of the thyroid gland (goiter)
- Change in menstrual cycles
- Erectile dysfunction or reduced libido
- Frequent bowel movements
- Bulging eyes (Graves' ophthalmopathy)
- Fatigue
- Thick, red skin usually on the shins or tops of the feet (Graves' dermopathy)
- Rapid or irregular heartbeat (palpitations)
- Sleep disturbance
Graves' ophthalmopathy
Graves' ophthalmopathy

Graves' ophthalmopathy
Graves' ophthalmopathy signs and symptoms include bulging eyes, redness and retracting eyelids.
About 30% of people with Graves' disease show some signs and symptoms of Graves' ophthalmopathy. In Graves' ophthalmopathy, inflammation and other immune system events affect muscles and other tissues around your eyes. Signs and symptoms may include:
- Bulging eyes
- Gritty sensation in the eyes
- Pressure or pain in the eyes
- Puffy or retracted eyelids
- Reddened or inflamed eyes
- Light sensitivity
- Double vision
- Vision loss
Graves' dermopathy
Graves' dermopathy

Graves' dermopathy
Rarely, people who have Graves' disease develop a reddish thickening of the skin that resembles the texture of an orange peel (Graves' dermopathy). This results from a buildup of protein in the skin. It often occurs on the shins and on the tops of the feet.
An uncommon manifestation of Graves' disease, called Graves' dermopathy, is the reddening and thickening of the skin, most often on your shins or the tops of your feet.
When to see a doctor
A number of medical conditions can cause the signs and symptoms associated with Graves' disease. See your doctor if you experience any potential problems related to Graves' disease to get a prompt and accurate diagnosis.
Seek emergency care if you're experiencing heart-related signs and symptoms, such as a rapid or irregular heartbeat, or if you develop vision loss.
Causes
Graves' disease is caused by a malfunction in the body's disease-fighting immune system. It's unknown why this happens.
The immune system normally produces antibodies designed to target a specific virus, bacterium or other foreign substance. In Graves' disease — for reasons that aren't well understood — the immune system produces an antibody to one part of the cells in the hormone-producing gland in the neck (thyroid gland).
Normally, thyroid function is regulated by a hormone released by a tiny gland at the base of the brain (pituitary gland). The antibody associated with Graves' disease — thyrotropin receptor antibody (TRAb) — acts like the regulatory pituitary hormone. That means that TRAb overrides the normal regulation of the thyroid, causing an overproduction of thyroid hormones (hyperthyroidism).
Cause of Graves' ophthalmopathy
Graves' ophthalmopathy results from a buildup of certain carbohydrates in the muscles and tissues behind the eyes — the cause of which also isn't known. It appears that the same antibody that can cause thyroid dysfunction may also have an "attraction" to tissues surrounding the eyes.
Graves' ophthalmopathy often appears at the same time as hyperthyroidism or several months later. But signs and symptoms of ophthalmopathy may appear years before or after the onset of hyperthyroidism. Graves' ophthalmopathy can also occur even if there's no hyperthyroidism.
Risk factors
Although anyone can develop Graves' disease, many factors can increase the risk of disease, including:
- Family history. Because a family history of Graves' disease is a known risk factor, there is likely a gene or genes that can make a person more susceptible to the disorder.
- Sex. Women are much more likely to develop Graves' disease than are men.
- Age. Graves' disease usually develops in people before age 40.
- Other autoimmune disorders. People with other disorders of the immune system, such as type 1 diabetes or rheumatoid arthritis, have an increased risk.
- Emotional or physical stress. Stressful life events or illness may act as a trigger for the onset of Graves' disease among people who have genes that increase their risk.
- Pregnancy. Pregnancy or recent childbirth may increase the risk of the disorder, particularly among women who have genes that increase their risk.
- Smoking. Cigarette smoking, which can affect the immune system, increases the risk of Graves' disease. Smokers who have Graves' disease are also at increased risk of developing Graves' ophthalmopathy.
Complications
Complications of Graves' disease can include:
- Pregnancy issues. Possible complications of Graves' disease during pregnancy include miscarriage, preterm birth, fetal thyroid dysfunction, poor fetal growth, maternal heart failure and preeclampsia. Preeclampsia is a maternal condition that results in high blood pressure and other serious signs and symptoms.
- Heart disorders. If left untreated, Graves' disease can lead to heart rhythm disorders, changes in the structure and function of the heart muscles, and the inability of the heart to pump enough blood to the body (heart failure).
-
Thyroid storm. A rare but life-threatening complication of Graves' disease is thyroid storm, also known as accelerated hyperthyroidism or thyrotoxic crisis. It's more likely when severe hyperthyroidism is untreated or treated inadequately.
The sudden and drastic increase in thyroid hormones can produce many effects, including fever, sweating, vomiting, diarrhea, delirium, severe weakness, seizures, irregular heartbeat, yellow skin and eyes (jaundice), severe low blood pressure, and coma. Thyroid storm requires immediate emergency care.
- Brittle bones. Untreated hyperthyroidism also can lead to weak, brittle bones (osteoporosis). The strength of your bones depends, in part, on the amount of calcium and other minerals they contain. Too much thyroid hormone interferes with your body's ability to incorporate calcium into your bones.