Feb. 08, 2024
Pinpointing the source of lumbo-pelvic stability issues typically requires conducting a comprehensive evaluation. According to Jane Konidis, M.D., a physiatrist at Mayo Clinic in Rochester, Minnesota, that evaluation should ideally include multiple key elements: testing the muscles in both the static and dynamic state, examining specific functions such as trunk control over a planted leg during a single leg stance or a squat, and evaluating multiple directions of motion, including three-planar activity.
"A typical evaluation in clinic for lumbo-pelvic stability can include careful observation of multiple types of movements, including these key tests: side-lying hip abduction, prone hip extension with knee flexed at 90 degrees and single-leg squat," explains Dr. Konidis. "If additional testing is required, you can incorporate static transversus abdominus and multifidus palpation and supine active straight leg raise with or without prone active straight leg raise and higher level dynamic testing as needed," explains Dr. Konidis.
Detailed instructions for performing a few of the more commonly used tests are outlined below.
Supine static contraction of the transversus abdominis muscle
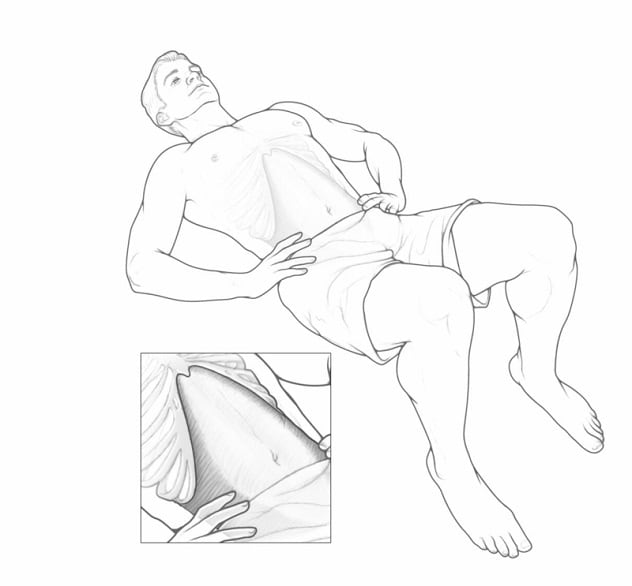 Engaging the transversus abdominis muscle
Engaging the transversus abdominis muscle
The transversus abdominus plays a critical role in lumbo-pelvic stabilization. To engage these muscles, ask the patient to draw in their navel, toward the back and upwards, as if a string is pulling on the navel. Tell them to imagine bringing both anterior superior iliac spine (ASIS) bones together toward the center of body, mimicking the muscle contraction used to stop flow of urination.
Ask the patient to draw in the navel, toward the back and upward, as if a string is pulling the navel. Tell the patient to imagine bringing both anterior superior iliac spine (ASIS) bones together toward the center of body, mimicking the muscle contraction used to stop flow of urination. During this test, the physician should palpate medially to ASIS. "The contraction should feel like a deep tension, with no 'bump,' " explains Dr. Konidis. "If a strong bump is felt (such as, for example, during coughing), then the obliques are compensating and engaging instead of the transversus abdominus muscle."
4-point kneeling static contraction of the multifidus
Sometimes it's easier for patients to activate the multifidus by contracting the transversus abdominus, especially if there's atrophy. To isolate the multifidus, ask patients to imagine drawing together both the posterior superior iliac spine (PSIS) or sacroiliac joint (SIJ), or to imagine drawing the knee and thigh into the pelvis.
"During contraction, the physician should palpate to the side of the lower lumbar spine," says Dr. Konidis. "Contraction of the multifidus should feel like a slow, firm swelling."
"A typical evaluation in clinic for lumbo-pelvic stability can include careful observation of multiple types of movements, including these key tests: side-lying hip abduction, prone hip extension with knee flexed at 90 degrees and single-leg squat."
Supine active straight leg raise (ASLR)
Originally developed for postpartum sacroiliac joint pain, the ASLR has been modified and expanded, and it is a good indicator of lumbo-pelvic stability. It can be tested with or without manual resistance.
- Part 1: Observe the hips anteriorly, watching for abdominal protrusion, rotation or extension of the lumbar spine, abdominal bracing maneuver, or the contralateral heel pushing down into exam table. Ask the patient if one side feels heavier than the other. Any of these signs could indicate that the patient is unable to use the deep inner muscles.
- Part 2: Transversus abdominis. The clinician squeezes the iliac crests together in antero-medial-upward direction, then directs the patient to lift the leg again. If this motion is easier or the leg feels less heavy, the patient may benefit from exercise(s) targeting the transversus abdominis and from the use of an SIJ compression belt.
- Part 3: Multifidus. Compress the iliac crest, directed posteriorly while pushing inferomedially, and ask the patient to lift the leg. If the patient says the leg feels less heavy or easier to lift during this maneuver, then the multifidus muscle is deficient.
- Part 4: Pelvic floor musculature. During compression of the greater trochanters, if the patient says the leg is easier to lift in ASLR, then the pelvic floor may be weak.
Prone ASLR
Begin by asking the patient whether one leg feels heavier than the other. Watch for evidence of compensatory mechanisms, including increased lordosis or extension in the lumbar spine, rotation of the pelvis, or use of the arm to push down into the exam table.
"This test is more focused on assessing the posterior sling, the latissimus dorsi and the gluteus maximus," explains Dr. Konidis.
- Part 1: Form closure. Patients with weaker core muscles typically find it easier to lift the leg while the iliac crest is compressed, directed medially.
- Part 2: Force closure. Ask the patient to lift the contralateral shoulder into extension and resist movement. If this is easier with resistance, the patient may benefit from exercise that targets the posterior sling.
Side-lying hip abduction with hip extension and slight internal rotation.
This movement targets the anterior fibers of the gluteus medius. During this test, patients with gluteus medius weakness may attempt to compensate by bringing their lower extremity more into flexion or with less internal rotation.
"This movement can also be used to evaluate coordination and lumbo-pelvic stability," explains Dr. Konidis. "Watch for pelvic tilting, trunk rotating posteriorly and increased lumbar lordosis as signs of this."
Single-leg squat — Frontal and sagittal planes.
- Frontal plane. If you observe hip or pelvis drop, or if the knee moves inward (valgus), this indicates weakness of gluteus medius with or without overactive adductors.
- Sagittal plane. Excessive trunk flexion or hyperlordosis during this movement also indicates lumbo-pelvic weakness.
For more information
Got glutes? Part 1 — The role of the gluteus maximus and healthy activation patterns in core stabilization
Refer a patient to Mayo Clinic.